E&M Coder Section
Disclaimer: The E&M Coder tool is intended for reference only. Users of the E&M coder must have an expert understanding of the E&M coding guidelines. The intended use of this tool is for you to calculate and validate your E&M code selection.
Providers:
In the Sign-off stage of the encounter, click the Billing tab, then click E&M Coder.
Administrative staff:
On the Claim: Billing tab in the Checkout stage, scroll down to the Services section to see confirmation of the E&M coder calculation.
To use the E&M coder, contact the CSC On the Main Menu, click Support > Success Community > Contact Client Support Center. Then request that the E&M Coder feature be enabled for your practice.
Evaluation and Management (E&M or E/M) codes, which range from CPT 99201-99499, represent services by a physician (or other health care professional) in which the provider is either evaluating or managing a patient’s health. (Procedures such as diagnostic tests, radiology, surgeries and other particular therapies are not considered evaluation and management services.) As such, they are some of the most widely used CPT codes and represent a significant portion of revenue for many providers. However, proper E&M code determination can be a complicated process of evaluating clinical data.
In 2021, the AMA simplified E&M guidelines in order to reduce administrative burden and improve consistency among payers. Determining the correct E&M code can now be done in two ways:
-
Evaluating the complexity of the encounter by determining the following:
-
Number and Complexity of the Problems Addressed
-
Amount and/or Complexity of Data to be Reviewed and Analyzed
-
Risk of Complications and/or Morbidity or Mortality of Patient Management
-
-
Calculating the total time spent on the encounter
What types of activities can count toward the total time?
According to the AMA guidelines, you can include the following time spent by the physician and other qualified health care professionals on the day of the encounter:
- Face-to-face time with the patient
- Preparing to see the patient (for example, reviewing tests)
- Obtaining and reviewing separately obtained history
- Performing a medically appropriate examination or evaluation
- Counseling and educating the patient, family, or caregiver
- Ordering medications, tests, or procedures
- Referring and communicating with other health care professionals (when not separately reported)
- Documenting clinical information in the electronic or other health record
- Independently interpreting results (not separately reported) and communicating results to the patient, family, or caregiver
- Care coordination (not separately reported)
To determine which code to use:
-
Choose a guideline. (The 2021 - Medical Decision Making guideline is automatically selected by default.)
-
Click the patient status. If athenaOne can determine that the patient is established based on historical billing data, the Established option gets selected automatically.
- If you choose:
- 2021 - Medical Decision Making — Select the values of all three Medical Decision Making questions. For more information on each question, you may review the 2021 guidelines on the side. Click the downward arrow to expand the associated guidelines for each question.
Time-Based Billing — Enter the total amount of time you spent associated with that visit on the date of service. (Refer to What types of activities can count toward the total time?)
-
Once you enter all of the information, athenaOne automatically determines the associated code.
-
Click Apply Code. The window closes and athenaOne adds the code the Billing Tab automatically.
-
To make further adjustments, re-open the E&M Coder where you can see all of the selected values and update as needed.
For Nursing Places of Service, you'll see different fields reflecting the needs of the associated code evaluation:
-
New and Established will not appear
-
A Visit Type (First, Subsequent visit, or Discharge visit) must be selected
Currently, the E&M Coder supports the following Places of Service:
-
Office (02, 03, 05, 06, 07, 08, 10, 11, 15, 17, 18, 19, 20, 22, 26, 49, 50, 62, 71, 72)
-
Home, residence and domiciliary (04, 09, 12, 13, 14, 16, 33, 55)
-
Nursing (31, 32, 54, 56)
We intend to support additional Places of Service in a future update.
Factors used to determine the E&M code include:
- The patient's status: New or Established
- The Place of Service of the service department
- Number and Complexity of the Problems Addressed
- Minimal
- Low
- Moderate
- High
-
Amount and/or Complexity of Data to be Reviewed and Analyzed
-
Minimal or none
-
Limited
-
Moderate
-
Extensive
-
-
Risk of Complications and/or Morbidity or Mortality of Patient Management
-
Minimal
-
Low
-
Moderate
-
High
-
Alternatively, if calculating by time:
- The patient's status: New or Established
- The Place of Service of the service department
- The patient's insurance: Medicare vs. non-Medicare
- The total time spent with the patient (Refer to What types of activities can count toward the total time?)
Certain Places of Service may also have unique factors. For instance:
-
For Nursing: Visit Type (First, Subsequent visit, or Discharge visit)
You can document the total time spent in each encounter for E&M billing through the Total Time Spent section of the Assessment & Plan (A/P).
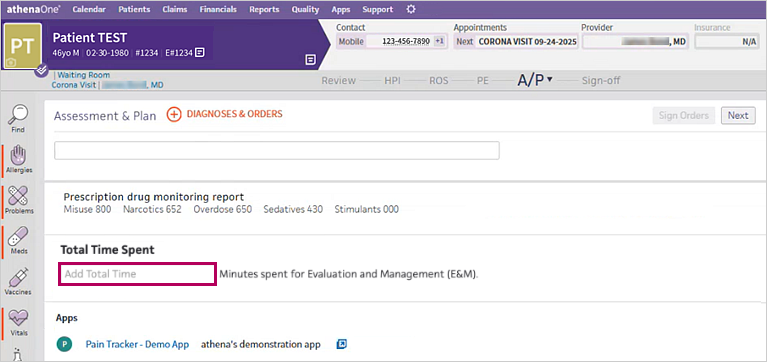
The Total Time Spent section is optional. If you leave this section blank, no total time spent information will appear in the encounter summaries.
All data recorded in the Total Time Spent section appears in the Sign-off stage in the following places:
-
Summary section
-
Full Encounter Summary
You can access the new Total Time Spent field across all encounter layouts, including the One-Stage Focused Visit.
For more information, refer to:
- Changes are coming to E/M coding; here's how we're preparing for January 1 — This web page explains what athenahealth is doing to prepare for the changes to E&M coding guideline for 2021.
- What's Changing for E/M Codes 99201-99215 in 2021? — This American Academy of Professional Coders (AAPC) web page provides an overview of what's changing in 2021.
- CPT Evaluation and Management — This AMA web page provides an overview and history of the changes, along with helpful resources and learning modules, including:
- CPT E/M Office or Other Outpatient and Prolonged Services Code and Guideline Changes — Review the CPT E/M changes that will go into effect on January 1, 2021.
- CPT E/M Office Revisions Level of Medical Decision Making (MDM) — This table helps you determine the appropriate level of MDM based on the modified criteria for MDM.
- 2020 Physician final rule — This CMS web page provides information about the updates to payment policies, payment rates, and other provisions for services furnished under the Medicare Physician Fee Schedule (PFS) on or after January 1, 2021.
| Encounter Type | |||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Place of Service |
Select the appropriate type of service value from the menu. Most often the provider will select outpatient consult, outpatient visit, and/or preventive management services.
|
||||||||||||||||||||
| Patient Status |
Review the patient status that the E&M coder section selects for your patient. athenaClinicals assumes the patient is "New" if it is unable to find clinical and/or billing records for the patient in your practice in the last three (3) years. |
||||||||||||||||||||
| Bill By Time? | Select this option if you want to bill by the amount of time spent with the patient. | ||||||||||||||||||||
| Total Time |
Time in minutes that the provider spent counseling the patient.
According to the AMA's updated CPT E/M guidelines, you can include the following time spent by the physician and other qualified health care professionals on the day of the encounter:
|
||||||||||||||||||||
| Medical Decision Making | |||||||||||||||||||||
| Overall |
According to CMS: Medical decision making refers to the complexity of establishing a diagnosis and/or selecting a management option as measured by:
The chart below shows the progression of the elements required for each level of medical decision-making. To qualify for a given type of decision-making, two of the three elements in the table must be either met or exceeded.
|
||||||||||||||||||||
| Dx/Management Options |
Refers to the complexity of establishing a diagnosis and/or selecting a management option. Select the value from the menu that best describes the diagnosis management options:
|
||||||||||||||||||||
| Complexity of Orders/Results |
Amount and/or complexity of data to be reviewed (Complexity of Data). Select the value from the menu that best describes the complexity of orders or results to be reviewed:
|
||||||||||||||||||||
| Problem Risk |
The risk of complications and/or morbidity or mortality. This is a composite of the following factors:
Select from the menu the value that best describes the problem risk:
|
||||||||||||||||||||
| Calculated CPT | |||||||||||||||||||||
|
The calculated CPT code appears here. |
|||||||||||||||||||||
| Notes |
Enter any notes about this E&M code. |
||||||||||||||||||||